Fangs
Imagine yourself leading a small group of adults and children through the thick cloud forest at Nectandra — all at once talking, walking and gently herding the children to stay on the trail. Your attention is split multiple ways — the subject matter, the ebullient children, spotting fauna and flora, where to land your feet and watching out for the coiled jumping pit viper that may become your next stepping stone. On two occasions, my feet came within 8 inches of the nearly invisible viperous bundle. I recoiled just in time in the first case and my companion yanked me sharply aside in the second. I don’t have a painful story to tell but the responsibility for guides to walk ahead became crystalline clear. Those seconds of terror also fixed my dread (and curiosity) of viper fangs.
Venomous distractions
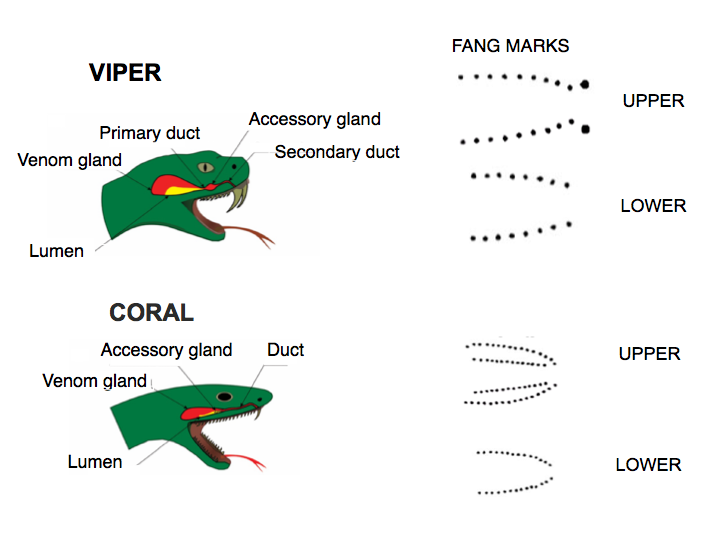
We all know about the danger of poisonous snake bites. We also know something about their venom and the availability of effective treatment using tailored antivenins. At Nectandra, elevation (1100 m, 3600 ft), pit vipers are more prominent than their better known cousin the fer-de-lance. The well camouflaged endemic jumping pit vipers (Fig 1 left) score the most bites requiring hospitalization in our area. The colorful, more timid coral snakes (Fig 1 right) have shorter fangs which may be loaded with neural venom, potent enough to be a source of worry for field workers and homeowners (I have caught several inside my house). Fortunately, our nearest hospital in San Ramon (15km) stocks antivenins to both snake groups.

While snake bites are professional hazards in the tropical forest, they are fortunately infrequent. Nevertheless, they are psychologically terrifying and medically serious. At our local hospital, the antivenin treatment requires two steps. If antivenin therapy is indicated, the first important step is to match the snake to the specific antivenin. The snake identity is determined from photos (thanks to cell phones), descriptions, physical specimens or from symptoms/appearance of the physical bites. If the snake identification is not possible (a very infrequent occurrence in Costa Rica), polyvalent antivenin to both the vipers and coral snakes is administered. In the second step, the patient is first infused with 1/10 of the final dose. If there is no detectable hypersensitivity to the associated horse serum, the infusion continues with the rest of of antiserum diluted in ≥40ml of saline. The whole procedure takes about 4-5 hours in the emergency room, followed by 3 days of observation.
Nationally, most (85%) of 500 annual snake bites are from the fer-de-lance (Bothrops asper). Coral snakes contribute ~2% of the bites. Even rarer are the bites from the jumping pit viper, an endemic snake found in mountainous, mid elevation region such as Nectandra. Unfortunately with a warming climate, the fer-de-lance has moved uphill and is now present at our cloud forest.
Why do snakes bite?
Snakes are able to carefully control the injection of venom. When threatened, 50% of the viper bites are “dry” bites with no or very small amount of the precious toxins injected, whereas most of the bites to kill prey involve venom. Hence, viper venoms are more for food and less for defense. In contrast, 85% of coral snake bites involve envenomation.
Anatomy of the jaws and fangs
Snakes swallow prey whole. Mechanically, it is not an obvious nor trivial task for them to bite/ingest large animals many times relative to its body size. First, let’s look at the jaw anatomy. Their specialized mandibles are not attached to each other, but to stretchy ligaments allowing their jaws to open very wide to accommodate very large prey. In vipers, the mouth expands, the two long fangs (Fig 2 top), which are normally folded inside the mouth, swing out (like a blade from a switch knife) and sink in to grab the struggling prey. The fang puncture marks and bite-associated physical symptoms are hallmarks of viper bites. Rows of backward-pointing, smaller teeth help the snake grab and pull in the prey. In comparison to the viper, the coral snake has smaller, shorter, fixed fangs, and multiple rows of upper teeth. In spite of their teeth, snakes do not chew their food. Vipers depend entirely on the fast acting digestive enzymes in their venoms to feed. In encounters with humans, viper bites are sharp and brief. Strike and release. In comparison, the less aggressive coral snakes may be more reluctant to bite, but when they do, they are slow to let go.
How is the venom delivered?
The venom is injected to paralyze, hemorrhage and break down tissues in prey. The snakes’ poison glands located behind their eyes are counterparts of the human’s salivary glands. The venom is specialized saliva containing a large cocktail of proteinaceous (> 50 enzymes) zootoxins. The venom is released from the system of glands through ducts under muscular pressure. It is injected much like liquid in a hypodermic needle and delivered through its hollow fangs under pressure of up to 30 psi (as in car tires). The size of the glands/ducts vary greatly, ranging from a few millimeters in length up to 1/4 of its length in the (old world) blue coral snake.
The vipers’ venom action in humans is rapid and intense. They may cause a combination of pain, welling, numbness, bleeding, bruising and blisters at the wound site (Fig 3). In comparison, coral venoms are neurotoxins and cardiotoxins . The smaller coral fang marks often are harder to see, painless with no swelling. The neurologic symptoms (drowsiness, nausea, headache, difficult breathing and paralysis) take longer to develop (up to 12 hours) but are then precipitous.

The best of fangs
The hollow, specialized teeth which we call fangs of the vipers (40 million yrs) and coral snakes (20-40 million yrs) evolved independently. As limbless animals, the snakes’ survival depend on their fangs, for both food and defense. The snakes’ successful radiation throughout the world attest to their fangs’ efficiency. Not only are snake venoms customized to their prey, but so are their fangs.
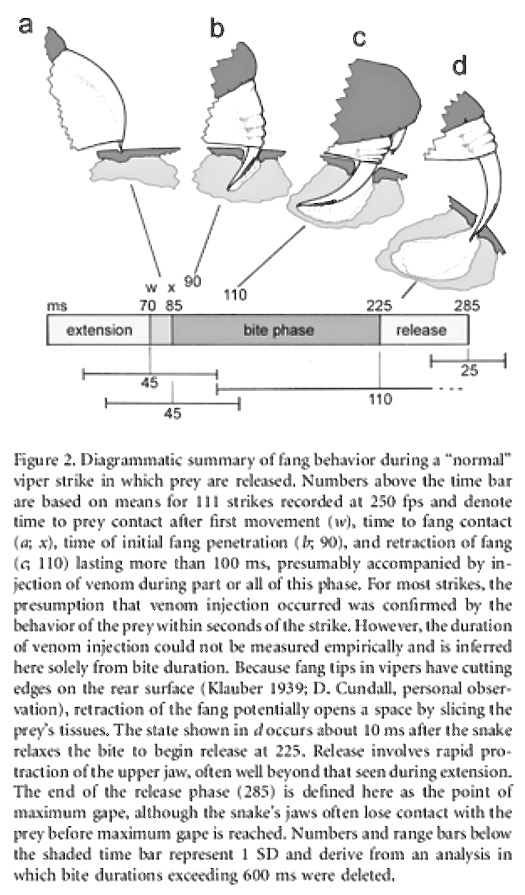
The fangs first task is to be able to penetrate the prey. The coral snake’s shorter and fixed fangs restrict the prey size. They must be able to bite through skins of reptiles, amphibians, insects and small mammals (e.g. scales, keratinized carapaces and furry skin etc). In contrast, vipers’ food may include all the above plus a wide range of large mammals and birds, varying in size, shape, hardness and textures. The complex mechanics of viper bites are being studied by a number of methods. For example, through time-lapse photography, the sequence of a viper bite when broken down into four steps, took place in an average of 285 milliseconds (about 3.5 bites per second) — during which time a small hole of the prey’s tissue was sliced open and the venom injected (Fig 4).
Newer technology such as microCT imaging reveals at high resolution the internal morphology and architecture of the fine bones and dentition structures in snakes (Fig 5).

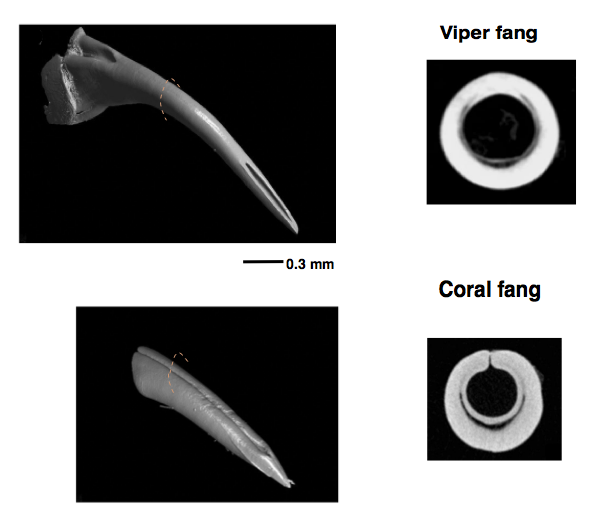
In general, viper fangs are very long and slender, with closed thinner walls that are more curved than coral snake fangs. The latter tend to be thicker, with the walls not completely fused — a characteristic of evolutionary trait shared by snakes related to coral snakes.
More intriguing are the differences in the angles and tips of the fangs. Sharp edges exist in all fangs. The viper has sharp edges along the top and undersurfaces, but only at the very tip. The coral fangs have small lateral ridges on each side of the fang (almost half way from the tip up) .
Mechanical stress tests using artificial metal punches mimicking snake fangs in varying shapes, length, angle and tip contours confirmed that the slender the fangs, the better the piercing. Not obvious, however, was that the sharpness of the fangs depends more on the tip angle and not its contour. A narrow fangs with blunt/rounded tip is a better performer than a wider fang with pointed tip. Ergo the fearful efficiency of the slender, curved and very sharp viper fans.
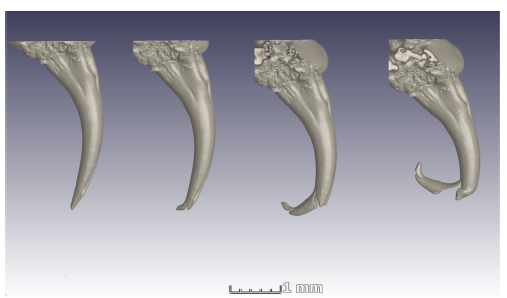
Fig. 7 is a series of microCT images showing what happened when the fangs were put under too much stress. To keep them sharp and ship-shape, fangs are replaced every two months.
The following is the link to an excellent (and astounding) case history of a coral snake bite, an ordeal suffered by this Colombian physician https://doi.org/10.1016/j.rcae.2016.02.010
Gilberto Villegas Velásquez (Givive)